Overview
José Antonio Izazola-Licea
Introduction
The appearance
of the Acquired Immune Deficiency Syndrome (AIDS) was described for
the first time in 1981 in the United States of America; unlike other
recent diseases (such as ebola), it has had a rapid dissemination
and a great social impact.
AIDS is the final
phase of the Human Immunedeficiency Virus (HIV), which may take from
5 to 20 years to manifest itself once individuals have been infected.(1)
Starting from the appearance of immunedeficiency and its manifestation
in "opportunistic" infections or in neoplasias, individuals can survive
up to two years even without antiretroviral or prophylactic therapy.
Survival can be increased in quantity and in quality by means of currently
available therapies.(2)
The AIDS pandemic
is composed of diverse, more localized epidemics, which have a dynamics
of their own and which, by bearing similarities according to regions,
can be characterized as epidemiological patterns. Initially, it was
thought that these patterns were explained essentially by differences
in sexual behavior and by the shared-use of needles and syringes during
the application of intravenous drugs. However, now other hypotheses
are proposed for explaining such differences; for example, the differential
transmission according to different HIV subtypes.(3) Differences have
also been noted in the composition of the epidemics according to the
early adoption of efficacious preventive measures, both in HIV sexual
and blood transmission.
AIDS already has
a place in history, not only because of its great negative impact
on health but also because of setbacks in gains on infant survival
in some countries. Indeed, part of the complexity of AIDS is that
it involves sexual behavior as one of the main routes of HIV transmission,
the latter being an area considered to be intimate and subject to
moral judgment by some. The appearance of AIDS has brought to light
some processes which socially influence the history of societies;
for example, the stigmatization of patients with terminal, chronic
or disfiguring diseases, such as bubonic plague, leprosy, syphilis,
and now AIDS. The fear of being affected causes some people to deny
the problem and to attribute it as a problem of others, frequently
resulting in decisions being made in non-ideal conditions.
Projection exercises
of the AIDS pandemic show a trend of accelerated growth in marginal
populations. In this way, what groups were the ones initially affected
is merely incidental: this epidemic, once mature, invariably spreads
more rapidly among vulnerable populations which have been traditionally
economically or socially marginal;(4) and it turns into an endemic
disease of heterosexual transmission, accelerated only because of
women’s lack of power in their relationship of equality to men
and by the discrimination toward other groups such as indigenous people,
homosexuals, widows, orphans, etcetera.
In 1996, scientific
advances made it possible to state, for the first time, the hypothesis
of control of the HIV infection by efficacious antiretroviral treatment;
however, this will be accessible only to a minority of persons, essentially
in industrialized countries, whereas it will be virtually unattainable
for the majority of the infected individuals in developing countries,
where currently 9 out of every 10 HIV infections occur. This situation
is little different to other efficacious alternatives of prevention
of perinatal transmission by the use of antiretroviral treatment at
the time of birth. The control of blood banks has demonstrated its
usefulness when one has had sufficient resources for its implementation;
however, its high cost and economic impact on health systems is clear.
The probable future emergence of a vaccine could also bring to light
the inequality among individuals and countries; once again, only those
with sufficient economic means will be able to rely on this preventive
tool.
The prevention
of HIV sexual transmission is based on a change in behavior; it is
now clear that community participation is indispensable for the sustained
change needed to alter the AIDS epidemic significantly, a process
linked to the democratic development of societies.
The continuing
growth of the pandemic, in addition to the change in the composition
of the affected, now leads to some people wanting to deal with AIDS
as an endemic problem, as acceptable as malaria or malnutrition, as
long as it is considered of other people’s bussiness. Unless
one implements an intense and well-directed strategy for the prevention
and the control of the HIV infection and one furnishes adequate comprehensive
medical care to the infected, the social and economic impact of AIDS
on health-care systems, and in general on societies, will be increasingly
greater. Indeed, health authorities should propose an effective combat
against AIDS, both preventive and curative, as part of the right to
health protection; however, the most efficient form should not necessarily
envisage the direct payment of governments of these activities.
In the light of
the advance of scientific and technological discoveries about HIV
and AIDS, of its pathogenesis and effective forms of fighting against
it, the most important question is no longer about the feasibility
of such discoveries, but about how to make them accessible to populations
who most need them. The question has ceased to remain solely in the
scientific and technological realm; it is now an economic question
as long as there are scarce resources available, and it is also a
political question in attempting to decide who will pay for the treatment
of the poor or the uninsured.
The costs of HIV/AIDS,
by the appropriation of resources in developing countries, characterized
by a scarcity of capital, are a matter of great importance in the
debate on economic development of Latin American and Caribbean countries.
The scarcity of economic resources, in turn, makes it imperative to
define priorities in governmental action. It is clear that the prevention
of HIV infection must be sufficiently financed, probably with public
funds, since it turns out to be a cost-effective intervention. Therapeutic
interventions, even though they are not considered to be cost-efficient
with the available information, should be carried out according to
the social security arrangements existing in each country; the uninsured
population, however, is the one that remains unprotected under these
schemes.
The changes in
the efficacy of antiretroviral or prophylactic treatments concerning
AIDS have been dramatic and frequent. Consequently, cost-efficiency
or cost-effective studies of the treatment become outdated. The higher
effectiveness of multiple antiretroviral treatments, which include
protease inhibitors, has produced an increase in the costs of standard
treatment for AIDS, but it has also modified radically the results
obtained with new therapeutic schemes. For this reason, one should
again evaluate the estimates of the cost-effectiveness ratio, in order
to be able to use adequately this information in the process of giving
priority to publicly funded actions, in a context of scarce resources
and multiple needs.
Virological
and Clinical Aspects of HIV
Background
Information on the Virus
When the first
AIDS cases in Latin America were diagnosed, little was known about
the disease. The causal agent had still not been identified, although
outbreaks of Kaposi Sarcoma and Pneumocystis carinii pneumonia
in homosexual and bisexual men with multiple partners were already
being described,(5,6) and cases among heterosexual couples, infants,
hemophiliacs, and receptors of multiple blood transfusions were being
reported. These studies supported the hypotheses of HIV sexual, blood
and perinatal transmission,(7-9) as the only efficient routes of transmission
which, so far, have been proved to exist.
The HIV is a retrovirus
of the Lentiviridae family, which were initially described
in feline and bovine pathologies. The first retrovirus described in
humans was the HTLV-I, in a form associated to a type of T-cell leukemia
in adults. In this way, the advent of technology to identify, isolate
and characterize the retrovirus of the 1960s permitted the speedy
description of the causal agent of AIDS, as well as the relatively
early development of methods of diagnosis and detection of HIV infection.
One of the characteristics
of HIV, which has implied greater difficulty for the discovery of
vaccines and possibly the development of viral resistance, is the
fact that the HIV has a large genetic variability and a high mutability,
which is very likely to have repercussions on the future of the epidemic
and on the design of strategies aimed at its control.
To date, two types
of HIV have been described, type 1 and 2. HIV-1 has, at least, 10
different viral variants or subtypes at the world level which are
designated with letters, from A to I, and group O. These subtypes
presented a regional pattern at the start of the epidemic, and now
they have disseminated. Thus, in Brazil and Argentina the HIV-1 subtypes
B, F and C have been described; in Mexico, the B, F and D subtypes;
and in Cuba basically the B subtype. Apparently HIV transmission is
differential by subtype, with the predominance of the E and C subtypes
for heterosexual transmission and the B subtype for homosexual transmission
and through intravenous drug use. HIV-2 has, apparently, a more benign
evolution than that of type 1 and possibly prevents the latter’s
infection by a crossed reaction. In order to face better the AIDS
epidemic, it will be necessary to know the subtypes and the characteristics
of the viral variants circulating in our populations. Although to
date the available techniques for the diagnosis of HIV infection (e.g.,
enzyme immunoassays (ELISA) and Western Blot techniques) are considered
to be high-precision diagnostic tools, it is important to establish
if viral variation affects the performance of these studies.(10)
Vaccines (I)
In spite of all
the knowledge acquired over the last few years about HIV, an available
effective vaccine does not yet exist. This fact is related with the
difficulties inherent to HIV, which had not been encountered previously
in the development of vaccines against other viral agents.
According to the
diversity found in HIV, the vaccines must be directed at the specific
subtypes circulating in the populations one intends to protect, and
most probably they must be polyvalent against various HIV subtypes.
Due to the absence of adequate animal models and to the results of
phase I and phase II clinical trials in humans, one should proceed
with phase III clinical trials to test the vaccines’ effectiveness.
However, multiple
problems remain to be solved before having a vaccine available for
its non-experimental use. A period of from 5 to 10 years must elapse
in order to evaluate if the vaccine effectively has a protective effect,
and that the disease has not been induced with the vaccine. Such evaluation,
in turn, must have a statistical design envisaging the adoption of
preventive measures, which by reason of ethics should be promoted
in exposed populations who are under a research protocol. To exemplify
this situation, a vaccine should be evaluated where there are high
rates of incidence in order to be able to detect significant differences
between the vaccinated and the non-vaccinated population; ethically,
one must promote the adoption of safe sex or condom use in these exposed
populations, which reduces the difference in the incidence of infection
among the vaccinated and the non-vaccinated population, thereby complicating
the process of evaluation of the vaccines’ effectiveness. Additionally,
one must take into consideration the circulating subtypes and the
specificity of such vaccines.
Studies are already
under way that take into account the route of HIV infection. Thus,
even though the importance of mucosal immunity has not been established,
independently of the type of vaccine used, the infection should probably
be prevented through these routes. Recent reports of new DNA vaccines,
currently under evaluation, induce an adequate mucosal response mediated
through IgA.
In addition to
the complexity in the development of vaccines, there continues to
exist a vacuum on immunological parameters which correlate with protection.
It is necessary, then, to have new methodologies of quantitative evaluation
of the cellular immunological function in order to asses the effectiveness
of the vaccines.
At the start of
the epidemic, when HIV was described as the causal agent of AIDS,
false expectations were raised concerning the early discovery of a
vaccine, leading, erroneously, to forecasting the end of the epidemic.
Population groups, in whom a significant change of behavior had been
achieved in the adoption of safe sex, soon forgot such practices,
thereby giving way to a new epidemic peak, for example, among homosexual
and bisexual men in the United States.(11)
Furthermore, it
has been recognized that the mere availability of a vaccine would
not be capable of containing the epidemic. Even if a vaccine were
currently available for field application, practical problems would
be encountered that would prevent its accessibility and utilization
with sufficient coverage to limit the problem of HIV infection: The
costs, the effectiveness and the acceptance of the vaccine could seriously
limit its utilization as occurs with other vaccines available since
a number of years ago, such as vaccines against measles, tetanus,
and hepatitis B. The solution to the growth of HIV/AIDS by means of
a vaccine will be more viable in countries having financial resources
to guarantee an adequate coverage.
Treatment (II)
During 1995 and
1996 important findings have been described in four main clinical
areas: HIV primary infection; virological markers to predict disease
progression and monitoring of therapeutic efficacy; treatment and
prophylactics of opportunistic infections; and antiviral therapy.(12)
The management
and pathogenesis of HIV primary infection have been the subject of
greater attention, in view of the evidence, increasingly greater,
that early antiretroviral treatment has a beneficial effect on the
subsequent clinical course of the infection; thus, one could recommend
the detection of individuals in the primary phase of HIV infection,
even before the occurrence of some immunological harm. However, this
perspective is still being debated owing to, among other causes, the
collateral effects of the antiretrovirals, the development of viral
resistance, and the high cost involved in maintaining antiretroviral
therapy over a prolonged period of time.
In the last few
years, methods have been developed to measure this viral replication
with enormous precision. These methods, which include the quantitative
detection of viral nucleic acids in plasma, have been recognized as
useful predictors of the long-term evolution of the HIV-infected patient.
The measurement of the viral load permits one to discriminate very
precisely patients whose velocity of progression will be different
in the long term; this measurement has also been used to evaluate
the response to antiviral treatment. Several studies have demonstrated
that the changes in viral load in response to treatment is associated
to a change in the prognosis, and therefore the viral load can be
used as a marker of the efficacy of antiviral treatment. Current recommendations
for managing an HIV-infected patient include the use of potent antiretrovirals
and monitoring its efficacy by means of viral load measurements.
As for opportunistic
infections, progress has been made in the evaluation of new prophylactic
schemes against different opportunistic infections, putting special
emphasis on the analysis of cost-efficacy. Trends in the prophylaxis
of opportunistic infections suggest the use of useful medication for
various infections, such as for example trimetropim-sulfametoxazole
for Pneumocystis carinii pneumonia (PCP) and also to prevent
toxoplasmosis. Furthermore, reports have been received of outbreaks
of multirresistant M. tuberculosis in hospitals in different parts
of the world, so that the use of multiple treatment against tuberculosis
is recommended, the combination of which is currently being evaluated
in seropositive patients. It is worth noting that attempts are being
made to simplify the administration of medication, while the use of
multiple prophylactic treatments with complicated administration schemes
only serve to diminish compliance to the therapeutic schemes.
Concerning antiviral
treatment against HIV, currently eight drugs have been approved in
the United States for use in HIV-infected patients. These are nucleoside
analogs (AZT, DDI, DDC, D4T and 3TC) and protease inhibitors (ritonavir,
indinavir and saquinavir). Other drugs are in advanced stages of evaluation
such as non-nucleoside reverse transcriptase inhibitors, nevirapine,
delarvina, and other protease inhibitors.
The use of a combination
of antiretrovirals is now the recommended practice, based on the results
on virologic markers that have been correlated to beneficial clinical
effects; therefore, the use of monotherapy should be discouraged.
The principles of current antiviral therapy should be based on achieving
a maximum virological suppression, for the longest period of time
possible and starting as early as possible. In the recommendations
of the International AIDS Society, issued in July 1996, emphasis was
put on the use of the viral load as a measure of effectiveness of
antiviral medication as well as for deciding on when to start its
administration.
Several schemes
in combination have been evaluated. Some of the most promising are
AZT / 3TC / indinavir or ritonavir; saquinavir / ritonavir; DDI /
D4T; AZT / DDI / nevirapine. The decision of using protease inhibitors
as the initial treatment is controversial and is not accepted in all
cases. The differences between protease inhibitors as to antiviral
activity, development of resistance, toxicity and interactions with
other drugs will be what determines the initial selection of one or
another. So far, there is no consensus over which is the recommended
protease inhibitor for initial use.
Given the advances
in the treatment of HIV infection, AIDS is on the way to becoming
a controllable chronic disease, by preventing the development of opportunistic
infections and even that of immunedeficiency. However, the degree
of complexity in the management of patients has increased substantially,
so that health-care models need to be planned taking into account
the patients’ prospects and the greater efficacy in the treatment.
The high degree of complexity suggests that the provision of medical
care to an HIV-infected patient should not be divided into primary,
secondary and tertiary levels of medical care.(13) Specialized medical
care should be provided from the early stages, which is when more
benefits can be obtained for the patient. Moreover, it should be considered
that to the extent that the immediate threat to life disappears from
view, the compliance to the treatment and the adequate use of medication
may be reduced, as has been observed in other potentially terminal
diseases (for example, diabetes mellitus).
It should be noted,
by way of conclusion about the advances in treatment, that the use
of combined therapies which include protease inhibitors, in spite
of having afforded very promising results over a 48-week follow-up
time period, does not constitute the "cure" against HIV infection.
The combined use
of antiretroviral drugs, of prophylactic medication and laboratory
tests for monitoring the advance of immunedeficiency (CD4+ cell count
and the quantity of viral load) represents a great economic cost in
the treatment of patients, which is out of reach for several health-care
systems. For this reason, and owing to the ethical relevance of providing
technologically available treatment, there is a need to search for
strategies to provide the greatest population coverage in the most
cost-efficient way possible.
The fact that
this technology is available should not be an excuse for neglecting
preventive activities; on the contrary, the obligation to provide
adequate treatment with high economic cost ought to be the best incentive
to prevent new HIV infections.
To foster the
increase in the coverage of anti-retroviral treatment, governments
may undertake diverse actions which do not necessarily imply large
expenditures. By way of example, central governments may, possibly
through their health ministries or charity agencies, effect massive
purchases of the medication, to guarantee the lowest prices. These
medications could then be sold at cost and the original expense would
be recovered; thus, patients and other agencies would have access
to lower-cost medications.
Epidemiology
of HIV/AIDS
The main aim of
epidemiology is to produce information for the action; it is used
to analyze the frequency and distribution of diseases and to identify
characteristics in the acquisition of the disease which can be modified
(risk factors). The adequate use of epidemiological information permits
one to describe which groups are more likely to acquire HIV as the
target population for interventions, or else it permits one to identify
practices as the objectives for behavior change which must be modified
to significantly alter the course of the epidemic. So far, it is recognized
that biological, social and behavioral factors have determined the
course of the epidemic. As a major cause of mortality and morbidity,
AIDS dramatically increases the burden on the health services and
diverts scarce economic resources for the treatment of patients, when
such resources could be used for preventive programs. All efforts
to characterize the HIV epidemic are directed at achieving the objective
of controlling this disease, reducing its social costs, and, additionally,
controlling its costs.(14)
Most HIV infections
and AIDS cases are occurring in developing countries in Africa, Asia,
and Latin America and the Caribbean. Recently, the epidemic has gained
momentum in the newly independent states of the former Soviet Union.(15)
Using the figures
estimated by the Joint United Nations Program on HIV/AIDS (UNAIDS),(16)
it is calculated that, since the beginning of the pandemic in the
1970s up to mid-1996, there would have been 7.7 million people in
the world who developed AIDS; 5.8 million who died from AIDS; and
27.9 million people who became infected with HIV.
In 1995 AIDS is
estimated to have caused 1.3 million deaths: of which 300,000 were
children, 400,000 were women, and 600,000 were men. Furthermore, by
mid-1996, 21.8 million people are estimated to be living with HIV
infection, still not diagnosed as AIDS. During 1996 there will be
3.1 million people newly infected with HIV¾ that is, 8,500 new infections
per day, the majority in persons aged 15-to-24, and 1,000 among children.
The increase in the number of reported cases from mid-1995 to mid-1996
was 19 percent.
The prevalence
of HIV infection is unequally distributed in the world: the highest
estimated prevalence among adults is in Sub-Saharan Africa (5.1%),
compared to Eastern Asia and the Pacific which have an estimated prevalence
of 0.01%, Latin America 0.5%, and the Caribbean 1.4% (see Figure 1
and 2).

Figure
1 Estimated distribution, as of mind 1996, of adults and children
infected with HIV since the late 1970s (global total: 27.9 million).
Source: UNAIDS/COS/SG/96017-1bw 30 June 1996.
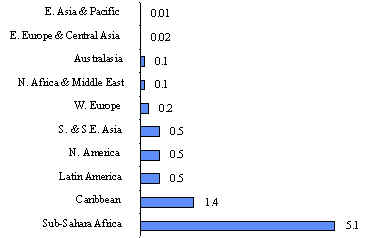
Figure
2 Adult HIV prevalence rates (%) by subcontinent, mid 1996.
Source: UNAIDS/COS/SG/96018-2bw 20 June 1996.
Epidemiology
of HIV/AIDS in the United States, Canada and Western Europe
In these regions,
more than 1.2 million adults are living with HIV/AIDS (including more
than 750,000 in the United States alone), which accounts for 6% of
the total number of cases in the world. At the beginning, the epidemic
in these countries affected homosexual and bisexual men. At present,
the epidemic involves largely injecting drug users and their sexual
partners, who may or may not be drug users. Up to 75% of infections
occur in injecting drug users or in their partners.
Ever since the
epidemic began, in the late 1970s, AIDS has come to rank as the number-one
cause of death in adults aged 45 or younger in many US and Western
European cities. In Western Europe currently around 450,000 people
are infected with HIV or have AIDS. There are indications that the
HIV prevalence has stabilized in countries such as Belgium, Germany,
the Netherlands, Sweden, and the United Kingdom. Switzerland has reported
a reduction in new AIDS cases, but the situation is less encouraging
in countries such as Spain, Portugal, and Italy.
Epidemiology
of HIV/AIDS in Eastern Europe and Central Asia
In Eastern Europe
and Central Asia, 29,000 adults are estimated to be living with HIV/AIDS.
Although this prevalence is still low, it is likely to increase since
the region has many factors conducive to a rapid dissemination of
HIV: economic crisis, rising unemployment, deteriorating health systems,
ethnic and religious conflicts, displacement of civil populations,
as well as migration in search of new economic opportunities. The
rate of infection is 15 per 100,000. Some countries have evidenced
a rapid spread of HIV infection, particularly Ukraine and Poland.
Epidemiology
of HIV/AIDS in Southern and Southeast Asia
The virus is spreading
rapidly and silently in most of Asia, the world’s most populated
region, especially in the southeastern part of the continent. Thus,
the total number of infected persons increased from 500,000 in 1991
to 3.5 million between 1991 and 1994, and to date a total of 4.7 million
adults are estimated to be living with HIV. The World Health Organization
(WHO) estimates that, by the late 1990s, the annual number of new
cases in the region will surpass that occurring in Africa, reaching
an accumulated total of 55 million people infected with HIV by the
year 2000; the WHO estimates, moreover, that by the end of the century
a total of 1.4 million people will have developed AIDS in Asia.
HIV was initially
identified in Asia among injecting drug users and in men with homosexual
practices. At present, while injecting drug abuse still plays an important
role in the spread of HIV, heterosexual transmission is the major
cause of infection in the region.
India is the country
with the largest number of infected adults with an estimated 3 million;
however, its prevalence in adults has not reached 1 %. Elsewhere,
Thailand is the country with highest prevalence in the area, with
slightly more than 2% among adults.
Epidemiology
of HIV/AIDS in Africa
The African countries
in the central, eastern and western areas to the south of the Sahara,
with less than 10% of the world’s population, account for more
than 70% of persons infected with HIV and more than two-thirds of
AIDS cases worldwide. Ever since the epidemic began in this region,
in the mid-1970s, around 13.3 million adults and over one million
children are estimated to have contracted HIV, and close to 3 million
people to have died as a consequence of AIDS. Most of the infections
have been acquired in heterosexual relations, with the number of infected
women higher than that of infected men. Approximately 8 million African
women in childbearing age are infected with HIV and one million children
have been infected before or during the time of birth or through breast
feeding.
There exists,
however, a wide variability in the AIDS-related incidence in Sub-Saharan
Africa. The prevalence of HIV ranges from 0.1% in the Comoros to 18%
in Botswana.
Life expectancy
at birth in the fifteen-year period of 1990-1995 decreased from 52.8
to 49.6 years in the 15 countries which had a prevalence of over 1%
in the population aged 15-49.
Epidemiology
of HIV/AIDS in Latin America and the Caribbean
Latin America
and the Caribbean have a relatively lower number of HIV infections
than Asia or Africa. However, and despite that Latin America and the
Caribbean represent 8.4% of the total world population, these regions
already contain 11.5% of all persons infected with HIV in the world.
The initial spread
of the HIV infection began in Latin America in the mid-1970s and the
early 1980s. Homosexual and bisexual transmission are estimated to
continue to be important in this region, but heterosexual transmission
is turning into the principal route of transmission. Sharing contaminated
needles and syringes among drug users is also a common route of HIV
transmission in many cities, especially in the South Cone of South
America. Between 1988 and 1992, the rates of infection in Latin America
and the Caribbean nearly tripled and towards the end of 1994 the region
had more than 2 million HIV infections and around 405,000 AIDS cases.
As in other regions
of the world, the AIDS epidemic in Latin America and the Caribbean
is becoming a high-priority public-health problem. The World Health
Organization and UNAIDS estimate that by 1996 there are a total of
1.6 million infected people living in Latin America and 300,000 in
the Caribbean. As of June 1996, a total of 176,930 AIDS cases were
reported in Latin America and the Caribbean. Nine countries (Brazil,
Mexico, Colombia, Venezuela, Honduras, Dominican Republic, Peru, and
El Salvador) account for 80% of the cases. Mexico and Brazil contribute,
altogether with more than 7 out of every 10 infections in Latin America,
18% of them in women. Overall, this region contributes 6% of the total
number of cases worldwide.
In the Caribbean,
there are more than 250,000 infections among adults; however, this
represents 1% of the world total, although the prevalence among adults
(1.4%) is surpassed only by that found in Sub-Saharan Africa. The
most affected countries are Haiti and Barbados with a prevalence among
adults of around 4%; the Dominican Republic and Haiti, taken together,
account for 85% of the total number of cases in the Caribbean. Cuba
is the country with the lowest prevalence (0.002%).
The AIDS epidemic
in Latin America has caused around 80,000 deaths and is on the way
to ranking as the major cause of death among men between 25 and 44
years of age. Because AIDS affects this important segment of the productive
labor force, its impact on productivity might be substantial. Determining
the size of the epidemic is critical because of its demographic, economic,
and public health implications.
Epidemiological Patterns in Latin America and the Caribbean
As for the distribution
of AIDS cases by mode of transmission, these may be classified into
the following three dominant trends:(17)
1) One characterized
by the predominance of transmission by male homosexual contact, followed
by sexual transmission and, finally, other categories (blood transfusions,
injecting drug users, etc.). This type of transmission is typical
of the Andean region: Bolivia, Colombia, Ecuador, Peru, and Venezuela
(see Figure 3), and, to a lesser extent, Mexico (Figure 4).
Figure
3 Annual incidence of AIDS cases, by certain risk factors, 1983/95.
Andean Area.
Source: Pan-American Health Organization HIV/AIDS in The Anericas,
January 10 update.
Figure
4 Annual incidence of AIDS cases, by certain risk factors, 1983-1994/95.
Mexico
Source: Pan -American Health Organization HIV /AIDS in the The
Americas, January 10 update
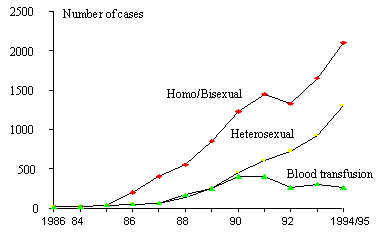
2) A variant of
the above-mentioned pattern is that of the South Cone (Argentina,
Chile, Paraguay, and Uruguay), where transmission is predominantly
among men who engage in homosexual practices, followed by a rapid
increase in intravenous drug users and by heterosexual transmission
(Figure 5). Brazil also has a similar behavior (Figure 6).
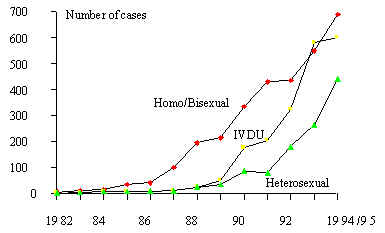
Figure 5 Annual incidence of AIDS cases, by certain risk factors,
1982-1994/95. Southern Cone.
Source: Pan-American Health Organization HIV/AIDS in The Americas,
January 10 update
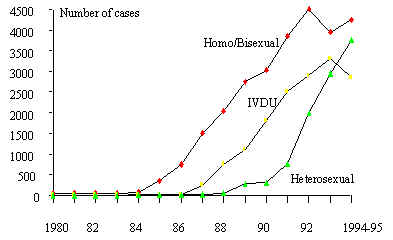
Figure 6 Annual incidence of AIDS cases, by certain risk factors,
1980-1994/95. Brazil.
Source: Pan-American Health Organization HIV/AIDS in The Americas,
January 10 update.
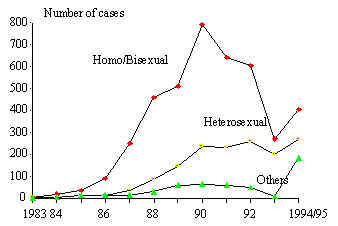
3) Finally, in
the Caribbean the main characteristic is predominantly related to
heterosexual transmission, in such a way that it has been compared
to patterns observed in the African continent (Figure 7). In Central
America (Belize, Costa Rica, El Salvador, Guatemala, Honduras, Nicaragua,
and Panama), particularly from 1990 onward, some authors have described
a "heterosexualization" of the epidemic, including a minority component
of male homosexual transmission (Figure 8). A dramatic example of
the high growth in cases related to heterosexual transmission has
been observed in Honduras, a country in which a total of 4,973 cases
and 955 deaths had been reported by the end of 1995.
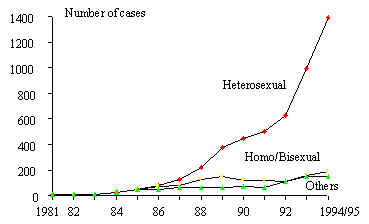
Figure 7 Annual incidence of AIDS cases, by certain risk factors,
1981-1994/1995. The Caribbean
Source: Pan-American Health Organization HIV/AIDS in The Americas,
January 10 update
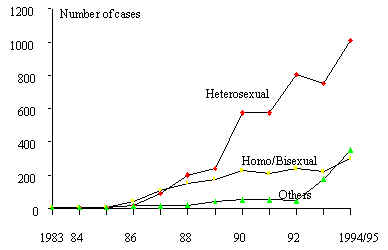
Figure 8 Annual incidence of AIDS cases, by certain risk factors,
1983-1994/95. Central America
Source: Pan-American Health Organization HIV/AIDS in The Americas,
January 10 update
Disability Adjusted Life Years lost due to HIV/AIDS and other STDs
A methodological
development exists that quantifies the burden of diseases by calculating
the Disability Adjusted Life Years (DALYs) lost including disability
and premature mortality.
This indicator
contains a discount of the future impact due to current infections,
and shows that in Latin America and the Caribbean the DALYs due to
HIV contributed with 10% of the transmissible diseases, maternal and
perinatal, and 25% of the infectious and parasitic diseases in 1990.
HIV/AIDS contributed the double of what was caused by maternal mortality
and the equivalent of 80% of what was contributed by acute respiratory
infections in the same year (Table 1).(18) Even though more recent
information is not available, the DALYs lost due to HIV/AIDS are expected
to increase to the extent that AIDS cases in the region have increased.
i.e., annual cases increased 10-fold in the period from 1990 to 1995
(in 1990, 15,651 AIDS cases were reported, and 155,169 cases were
reported in 1995).
Table
1. Disability-adjusted life years (DALYs, in thousands): Latin America
and the Caribbean
| |
Both
sexes
all ages
|
Males
|
Females
|
| ALL
CAUSES |
102,892
|
57,218
|
45,674
|
| Communicable,
maternal & perinatal |
43,415
|
22,649
|
20,766
|
| Infectious
& parasitic diseases |
25,851
|
13,783
|
12,067
|
| STDs
excluding HIV |
2,403
|
244
|
2,159
|
| HIV
infection |
4,435
|
3,414
|
1,021
|
| Noncommunicable
|
44,030
|
22,847
|
21,183
|
Because of the
natural history of the disease¾ which indicates that up to 20 years
may elapse between the infection with HIV and the clinical diagnosis
of AIDS,(7) even without prophylaxis and antiretroviral therapy¾ the
presence of early symptoms not diagnostic of AIDS, the psychological
burden of knowing to be seropositive, and to the average four-year
survival period once diagnosed with AIDS, the burden of the disease
corresponding to HIV/AIDS should be measured not only as mortality,
but also as morbidity and disability.
Life years lost due to premature mortality caused by HIV/AIDS
By the end of
1995, there were a total of 388,633 deaths caused by AIDS in the American
continent; of these, 311,000 occurred in the United States, 36,024
in Brazil, and 14,167 in Mexico.(19)
In Mexico, the
mortality caused by AIDS has gained ground within the major causes
of death among young men: in 1988 AIDS ranked eleventh as the cause
of death among men aged 25-34; in 1992 it ranked fourth;(20) and currently
it ranks third (Figure 9).(21) Several studies have noted, moreover,
that such data can still be corrected. By way of example, in the United
States the mortality recorded directly as AIDS needs a correction
factor. An study conducted in San Francisco, California, indicates
that 9% of the deaths due to AIDS were not directly recorded as such
on the death certificate;(22) a United Sates national study suggests
that a correction of 26% needs to be added to the recorded number
of AIDS deaths occurring among men in the age group 25-44.(23)
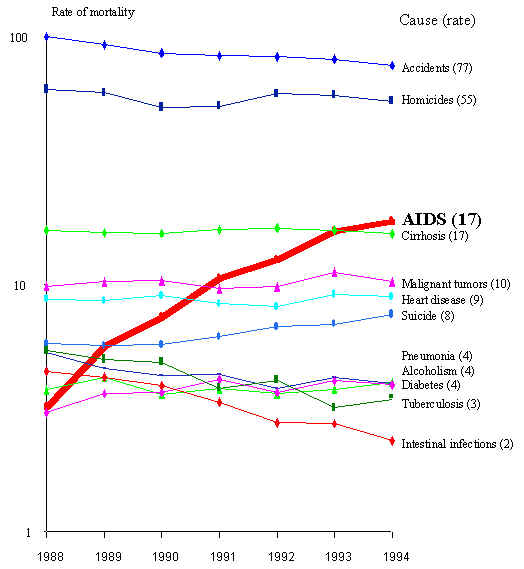
Figure 9 Rate of mortality (per 100 000 inhabitants) of the main causes
of death in men , ages 25-34
In Mexico, preliminary
results of a study(3) indicate that the mortality rate in young men
(age 25-44) should increase by 30% owing to this process of inadequate
certification. For example, for 1994, of the cases not certified as
HIV/AIDS which are ascribable to this cause, 37% were classified as
meningitis caused by enterovirus; 7% as tuberculosis; 12% as pneumonia;
5% as virosis of the central nervous system; 4% as anemia; 13% as
missclassified bacterial infections, etc. The major conclusion in
using this correction is that mortality due to AIDS contributes 12%
of the total mortality in this group in Mexico. This process of miss-classification
of the cause of death may occur because physicians involved in treating
such patients do not record HIV/AIDS as the cause of death.(24) It
is to be expected that a similar process is occurring in the rest
of the region.
Prevention
of HIV(III)
The subtypes recognized
to be circulating in Latin America and the Caribbean and the biological
variability of HIV have the potential to produce new sub-epidemics
in the region. For example, if the hypothesis of a subtype with a
greater efficiency for heterosexual transmission is proved correct,
and considering that this subtype has not yet circulated in the American
continent, and considering that about 10 million adolescents annually
initiate sexual activity, clearly there is a potential for a latent
heterosexual epidemic.
While the new
viral characterization will make it possible to monitor the geographical
distribution of sub-epidemics, it also has important implications
for the development of a vaccine. Any vaccine, to be efficient, must
induce immunity that recognizes the envelopes of the different subtypes,
as has been mentioned previously in this chapter. However, in spite
of the identification of these subtypes, in terms of prevention of
HIV sexual transmission, one thing should remain very clear: protected
intercourse continues to be the best way to prevent the spread of
the HIV regardless of its subtype.
Sustained efforts
to maintain continuing campaigns for protected sexual intercourse
and condom use are necessary. Although it is true that governments
are responsible for the provision of preventive and health-care services
for the population, community involvement and participation are essential
for the success of preventive interventions to control the AIDS epidemic.
Concerning the
prevention of HIV/AIDS infection, it is known that information, education
and communication models designed to promote awareness among the public
at large of the existence and the mechanisms of HIV transmission have
not led to changing HIV-risk behaviors. To state it once again, there
is no linear and direct relationship between knowledge, attitudes,
and practices. Information does not suffice to prevent AIDS. Preventive
interventions should not only change individual behaviors in an isolated
manner from other underlying conditions; HIV/AIDS-risk behaviors in
vulnerable populations are entrenched in broader contexts which determine
them.(25)
The determination
of preventive programs is based on the identification of factors that
are associated with an increased risk of acquiring HIV infection.
When these factors are susceptible to being changed, then one can
plan and assess programs to prevent infection. In the case of HIV
infection, having unprotected (without condom) sexual intercourse
is still the most important risk factor for acquiring the infection.
Up to now behavioral factors and social networks had been considered
to be much more important elements in spreading the epidemic than
the biological factors of the virus. The success of community programs
is based on a design sensitive-to-the-needs and customs of the targeted
communities, as well as on the participation of persons who are part
of the same community. The presence of sexually transmited infections
is associated to a higher risk of HIV transmission; for this reason,
one should stress their treatment and widely prevent them by the use
of condoms. Two strategies for providing information on HIV and promoting
the consistent use of condoms include interventions aimed at mass
media and those directed to specific groups, i.e., face-to-face interventions..
For other routes
of transmission such as parenteral, the self-exclusion of blood donors
at risk of being infected, the prohibition of blood commerce and the
universal screening of blood donations with the elimination of infected
products have been successful for controlling the transmission by
blood transfusion, to the point in which blood transmission cases
have been significantly reduced. (Figure 10)
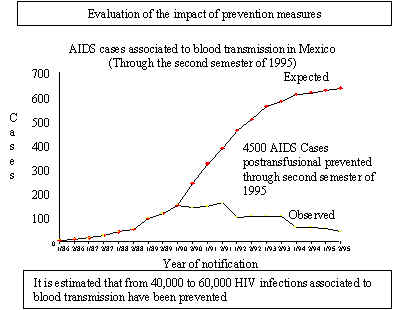
Figure 10 Prevention strategies in Mexico
Cases of HIV infection
related to injecting drug use in Latin America- located in urban areas
such as cities on Mexico’s northern border, Rio de Janeiro,
Brazil, and Buenos Aires, Argentina- require intense intervention.
One of the most
promising areas of prevention is in perinatal transmission. At present,
the standard care for pregnant HIV-infected women includes zidovudine
administered to the mother shortly before, during and to the baby
after the partum, since it is able to reduce transmission in two thirds
of the cases, i.e., from an estimated 24% to an estimated 8%.
Social Vulnerability, Human Rights and AIDS
During the past
decade important changes have taken place in the research on the social
impact of HIV/AIDS and on a critical reflection about the epidemic,
both from the point of view of political theory and of practical experience.
Such is the case of studies that attempt to understand and attack
the social, economic and political determinants of the epidemic, as
well as innovative designs of preventive interventions based on the
understanding of AIDS as a social problem that must be dealt with
from a community level.
These changes
are based on several issues. Although the universal biological susceptibility
to HIV infection is true, the epidemiology of the infection shows
that certain groups are more vulnerable because of their social, economic
and cultural conditions, such as women, youngsters, the poor both
in developing countries and industrialized societies, and groups that
have been stigmatized for their sexual practices such as men who have
sex with men. Hence the reason why the concept of "social vulnerability"
regarding HIV infection has gained great importance and why the need
to direct research and prevention efforts toward broader areas than
individual behavior change is being discussed.
The major challenges
that AIDS implies in our societies lie not only in the prevention
of blood, sexual and perinatal HIV transmission, but also include
reducing the impact of HIV infection on individuals, on groups, and
on societies. Other challenges include the provision of health care
for AIDS patients, the stigmatization of the affected and their families,
and the complacency in regard to a disease which, according to some,
is already an "acceptable" cost of living in modern times.
Because fighting
against HIV/AIDS requires and will require sizable economic resources,
the inequity among countries, societies and individuals adds a degree
of difficulty, given our Latin American reality.
In fact, AIDS
has uncovered the greatest weaknesses of our societies, by making
us reflect on the identity and the behavior of the affected persons
and, necessarily, showing us the existing diversity from way back.
We have had to face in an explicit manner the need to respect individuals
who do not think or do the same as "us" and who, however, share our
same rights. The rich and the poor, housewives and homosexual men,
prostitutes, drug users and adolescents will have those same rights.
The same rights as citizens and the same human rights.
Tolerance existing
before the onset of AIDS, for example in sexuality, was transformed;
thus, some became more intolerant and others are now respectful of
the human diversity.
Despite that in
some countries the initially affected groups were those who enjoyed
better economic conditions, at the world level it has been observed
that the HIV/AIDS pandemic affects inexorably, and increasingly, individuals
with greater vulnerability. This vulnerability is due to biological
conditions, economic situations, sexual practices, or a combination
of these and other situations. In other words, on account of being
a woman, of being poor, of being homosexual, of being a migrant, of
being a prostitute, of being a drug user, or of being a housewife.
It is clear that an effective response for fighting against this disease
demands the mobilization of society, both through governments and
civil society itself.
The affectation
of women by the HIV/AIDS epidemic has been unequal in the world; while
in Sub-Saharan Africa and the Caribbean the number of affected women
is equal to or slightly higher than the number of affected men, in
Latin America women account for only 18% of the cases. Worldwide,
by mid-1996, 12.2 million adult men and 8.8 million adult women are
estimated to be living with HIV.
However, the conditions
of women¾ particularly owing to their state of inequality in decision-making
and in social participation, as well as because of their biological
characteristics¾ cause them to become a vulnerable population for
acquiring HIV infection, essentially due to actions taken by their
male partners, often in spite of being aware of the risks involved
for women and their children.
In this sense,
it is urgent to undertake research on women, from a gender perspective,
about the lack of perception of risk for HIV/AIDS, of the obstacles
for negotiating safer sexual practices, and about the role of different
social institutions as favoring or hindering the campaigns aimed at
fighting against AIDS. Among the most urgent proposals to stem the
epidemic, primarily among women in the region, are the following:(26)
Include specific
educational messages for women.
Achieve the production,
distribution and wide accessibility of the female condom and other
methods of protection controlled by women.
Broaden the coverage
and the accessibility of comprehensive childbearing health services,
which should include AIDS prevention actions and the detection and
treatment of their sexually transmitted diseases.
Economic Impact of HIV/AIDS
Impact of HIV/AIDS
on the Economy(IV)
When AIDS first
appeared at the beginning of the 1980s, it was primarily considered
a public-health problem. However, because HIV infection was associated
to determined sexual practices, in some countries there was the dilemma
of regarding AIDS as an ethical or moral question or as a public-health
question. Clearly, the discussion of that dilemma distracted from
giving attention to the central points of the problem, and currently,
in addition to being a public-health problem, AIDS has become a concern
for economic development.
In fact, the evolution
of HIV/AIDS is adversely affecting development. In the long term,
productivity (production per worker) is nearly all that matters for
economic development. The capacity of a country to improve its standard
of living over time depends almost completely on its ability to raise
its production per worker. To be fair, and as a purely arithmetic
question, at least in a closed economy, there are three ways of increasing
a country’s per capita consumption: a) increasing productivity,
so each worker produces more; b) putting a larger portion of the population
to work; and c) putting a smaller fraction of a country’s output
aside as investment for the future and devoting more of the country’s
productive capacity to manufacturing goods for current consumption.
AIDS certainly affects the three ways to increase a country’s
per capita consumption, because, by being a disease, it implies less
working days, lesser opportunities to obtain better-paying jobs, and
shorter working lives.(27)
It should be pointed
out that AIDS has a much lower prevalence in developing countries
than other diseases such as malaria, but its economic impact by case
is greater for several reasons, among them, the following:
1) It mainly affects
adults in their most productive years.
2) The infections
resulting from HIV/AIDS lead to heavy demand for expensive treatments.
3) To the extent
that the treatments fulfill their task, their prescription could be
prolonged for lengthy periods.
4) The number
of persons already infected with HIV who have still not developed
AIDS is already of huge proportions (nearly 22 million people worldwide
in 1996).
5) The number
of HIV-infected persons is likely to continue to increase.
The relationship
between underdevelopment and health is quite well known when talking
about other pathologies. Concerning AIDS, not only do relationships
exist which explain the greater growth in poor countries and marginal
populations, but also deficient reactions are conditioned in facing
the problem. The long history of poverty in the most affected countries
makes one think that, even if the cure of AIDS should solely consist
in drinking potable water, a large quantity of persons¾ mainly in
developing countries¾ would not have access to that treatment.
The probable impact
of AIDS on economic development has been debated at length. Thus,
a common argument is that the economic impact of AIDS on developing
countries does not really constitute an economic problem because ill
or dead workers will be replaced by unemployed persons, owing to the
abundance of cheap labor and high unemployment. This argument may
be valid as long as there exists sufficient unemployed persons who
wish to replace those who can no longer work due to AIDS. But even
in countries with the highest unemployment rates, the labor "reserve
army" is bound to disappear in the presence of a disease for which
no cure exists, as is the case of AIDS. In the presence of a disease
like AIDS, full employment could finally be achieved. However, if
the cure continues to be non-existent or prohibitively expensive for
developing countries, and if the number of AIDS cases grows more rapidly
than the labor force, what would follow? Then, production will be
negatively affected, since the labor force in the full-employment
economy will begin to decline, with adverse consequences on social
welfare.
The HIV/AIDS epidemic
has a heavy macroeconomics impact, owing in part to the high costs
of treatment which divert resources from productive investments. More
specifically, the costs of HIV/AIDS are commonly classified as: a)
direct, which are the costs of personal- and health-care that
an infected individual needs, including non-personal services such
as blood screening, health education, staff training, and research;
b) indirect, which are the costs in terms of lost production
due to morbidity and mortality caused by AIDS, including estimates
for the value of unmarketed production, such as housekeeping tasks
and subsistence agriculture; c) direct invisible costs, represented
by services provided by family, friends and charities; although unpaid,
these services represent a real consumption of resources, and hence
a real cost, and their omission can lead to suboptimization in choosing
between different care strategies; and d) indirect invisible costs,
which are the costs of intangible reactions and lower quality of life
through factors like pain, incapacity, fear, anxiety, isolation, stigma,
depression, etcetera; these costs are obviously important in the case
of AIDS, but it is very difficult to estimate them.
The potentially
devastating effects of the HIV/AIDS epidemic can be averted with relatively
modest resources. In fact, a country does not have to be rich to be
successful in prevention efforts. The desirability of prevention in
the case of HIV/AIDS is considerably important given the vast benefits
of preventive action and the enormous future costs incurred in the
absence of it. Since there is no vaccine or cure for AIDS, prevention
is the only way to fight the epidemic.
Prevention involves
relatively low costs and, if effectively implemented, yields enormous
benefits. The World Bank reports that studies conducted in nine developing
and seven industrialized countries suggest that preventing a case
of AIDS saves, on average, an amount equivalent to about twice the
GNP per capita in discounted lifetime costs of medical care, and in
some urban areas the savings may be as much as five times the country’s
GNP per capita. The benefits of prevention must also take into account
that in the case of communicable diseases, and especially of epidemics
like HIV infection, estimates must take into account the fact that
each case prevented also prevents subsequent cases.(28)
The urgency of
increasing prevention efforts becomes evident when we look at the
projections available, which indicate that the HIV/AIDS epidemic has
disastrous consequences that get worse with the passage of time.
From an economic
standpoint, it is of utmost importance to increase without delay the
prevention efforts, which involve a very modest cost when compared
with the direct costs of an uncontrolled HIV/AIDS epidemic. The decision
maker has the alternative of acting now using relatively little resources,
or suffer tomorrow, having to use considerably higher amounts of resources.
The costs of HIV/AIDS, by diverting scant resources in developing
countries¾ precisely characterized by a scarcity of capital¾ are a
matter of considerable importance.
In the United
States, in 1991, the average annual cost of the medical-care management
of each one of the AIDS cases was estimated to be US $38,000; assuming
an increase in the annual cost of medical treatment of AIDS patients
of 7 to 8% annually, for 1995 the annual cost per case would be US
$120,000.(29)
For example, in
1991 it was found that the use of zidovudine in a patient without
symptoms, a cost-effective intervention, since it prolongs life expectation
and has a cost of approximately US $6,600 per life year gained, which
compares favorably with other routine medical interventions such as
heart surgery.(30)
Of the direct
costs, the hospitalization cost¾ at the beginning of the epidemic¾
represented the greater part of the medical-care cost for AIDS patients.
To the extent that ambulatory medical-care schemes are adopted, the
costs of medications will account for the greater part.(31)
The direct cost
of using three antiretrovirals¾ for example, AZT, DDC and saquinavir¾
could reach in Mexico, in mid-1996, an annualized cost of US $17,336.
The cost of using prophylactic medications for other microorganisms
would correspond to more modest amounts; for example, an annual US
$50 for trimetroprim-sulfametoxazole used for the prophylaxis of P.
Carinii and Toxoplasmosis, and US $800 for the use of azithromicin
for the prevention of Mycobacterium avium. The use of prophylaxis
varies according to the condition of the patients; however, often
multiple medications are used for the prevention of opportunistic
diseases, whereupon the cost of each prophylactic medication should
be added to the list of direct costs involved in the provision of
medical care for the affected.
It should be clear
that the lack of an explicit medical care policy for AIDS patients
or for the prevention of HIV infection does not imply that this epidemic
will cease to cause expenses, both in the economy of countries and
in health systems. In fact, the lack of a medical care and prevention
policy for HIV/AIDS often is one of the most expensive strategies
to face it. Indeed, the fact that persons who now become infected
with HIV do not develop AIDS until many years later does not free
today’s public-health authorities from their responsibility.
Expenditure
on HIV/AIDS in Mexico, a case study
In an accounting
exercise of amounts spent in Mexico for 1995, a study was carried
out to provide a panorama of the estimated global amount of expenses
by type and by source.(32,33) The mechanism for these estimates consisted,
firstly, in the identifación of the institutions providing health-care
for HIV/AIDS patients, the population covered by them, health-care
and prescription patterns, and the funding sources of these institutions;
also, preventive actions were listed, in addition to estimating their
cost and financing source.
In broad terms,
HIV/AIDS-related expenses were estimated to have amounted to US $79.1
million for 1995. The majority of these expenses were recorded in
the item of medical care (85%) and in public sector expenditures.
International contributions accounted for 1% of total expenses in
this item and were earmarked essentially for prevention (Tables 2-4)
Table
2. Overall Health Expenditures by type and source of funding
Preliminary Estimates. Mexico, 1995. (million USD)
| |
Domestic
Public
|
Domestic
Private
|
International
|
TOTAL
|
| Prevention
|
578.1
7%
|
86.0
1%
|
57.8
1%
|
721.9
9%
|
| Treatment
|
5,331.0
65%
|
1641.0
20
|
28.9
<1%
|
7,000.9
85%
|
| Mitigation
|
467.6
6%
|
0
0%
|
0
0%
|
467.6
6%
|
| TOTAL |
6,376.7
78%
|
1727.0
21%
|
86.7
1%
|
8,190.4
|
Table
3. Overall HIV/AIDS Expenditures by type and source of funding
Preliminary Estimates. Mexico, 1995 (million USD)
| |
Domestic
Public
|
Domestic
Private
|
International
|
TOTAL
|
|
Prevention
|
16.6
21%
|
11.9
15%
|
0.9
1%
|
29.4
9%
|
|
Treatment
|
24.0
30%
|
25.4
32%
|
0.0
0%
|
49.4
85%
|
|
Mitigation
|
0.2
<1%
|
0
0%
|
0
0%
|
0.2
6%
|
|
TOTAL
|
40.8
52%
|
37.3
47%
|
0.9
1%
|
79.1
|
Table
4. % Expenditures on Health and AIDS
| |
Domestic
Public
|
Domestic
Private
|
International
|
TOTAL
|
|
Prevention
Health
AIDS
|
7%
21%
|
1%
15%
|
1%
1%
|
9%
37%
|
|
Treatment
Health
AIDS
|
65%
30%
|
20%
32%
|
<1%
0%
|
85%
62%
|
|
Mitigation
Health
AIDS
|
6%
<1%
|
0%
0%
|
0%
0%
|
6%
<1%
|
|
TOTAL
Health
AIDS
|
78%
52%
|
21%
47%
|
1%
1%
|
8,190.4
79.1
|
Expenditures on
prevention
In terms of prevention,
spending amounted to approximately US $29.5 million. The expenses
can be classified into the following two categories: blood-bank screening
for the prevention of HIV blood transmission (US $16.4 million); and
expenses on prevention of HIV sexual transmission (US $13 million).
Blood-bank screening expenses were essentially charged to public expenditure
(US $11 million), divided in equal parts among social security institutions
(IMSS and ISSSTE) and, a lower amount (US $5.3 million), was spent
by civil and private institutions, among them, mainly the Mexican
Red Cross. (Table 5).
Table
5. Prevention expenditures by type and source
Mexico, 1995
| |
TOTAL
|
I,E
& C
|
Blood
Bank Screening
|
Condoms
|
| DOMESTIC
PUBLIC |
16.6
(56%)
|
5.5
(19%)
|
11.1
(38%)
|
0
(0%)
|
| Direct
Government |
7.8
(26%)
|
2.3
(8%)
|
5.5
(19%)
|
0
|
| Social
Security |
8.8
(30%)
|
3.2
(11%)
|
5.5
(19%)
|
0
|
| DOMESTIC
PRIVATE |
11.9
(40%)
|
4.0
(14%)
|
5.3
(18%)
|
2.6
(9%)
|
| Out
-of- Pocket |
2.9
(10%)
|
0.3
(1%)
|
0
|
2.6
(9%)
|
| Private
Insurance |
0
(%)
|
|
|
|
| Employer
|
3.2
(11%)
|
3.2
(11%)
|
0
|
0
|
| Non-Government
Organization |
5.8
(20.
0%)
|
0.5
(2%)
|
5.3
(18%)
|
0
|
| INTERNATIONAL
|
0.9
(3%)
|
0.8
(3%)
|
0
|
0.1
(<1%)
|
| TOTAL |
29.5
(100%)
|
10.4
(35%)
|
16.4
(56%)
|
2.7
(9%)
|
The federal budget
was the main source of expenditures on prevention of HIV sexual transmission.
Additionally, non-governmental organizations provided, in an important
way, services for the prevention of AIDS. The latter were considered
as non-monetary expenses, given their difficult quantification, the
difficulty in establishing their coverage, since such services are
largely based on donations and on non-paying voluntary work.
Governmental expenditures
for the prevention of HIV sexual transmission were estimated using,
primarily, the budget of the National Council for the Prevention and
Control of AIDS, which is the governmental agency with that specific
mandate. It was not possible to identify other governmental financing
sources for HIV sexual transmission prevention activities. However,
upon the conclusion of the decentralization of the Health Secretariat,
the respective funds are expected to be transferred, as, likewise,
the responsibility for the planning and the implementation of these
activities.
It should be noted
that public outlays on information, education and communication were
primarily financed through public expenditure (US $16.3 million),
through private funds (US $11.9 million), and through contributions
from international organizations (US $0.9 million). Of this total,
direct out-of-pocket consumer expenses were estimated to be US $2.6
million, for direct purchase of condoms. Expenditures through non-government
organizations were not easily quantified, and were not included in
this estimate.
Expenditures on
medical care
Given that medical-care
outlays are not found available in any official source, these were
estimated by establishing typical patterns of treatment for typical
patients, by service providers (physicians) who cared for the highest
proportions of patients. The cost of each treatment pattern was estimated
using the average costs for each service; e.g., hospitalization day,
medications, medical consultation, laboratory tests, etcetera. Finally,
the cost of each treatment pattern was multiplied by the estimated
number of patients in each health-care center of each institution.
The resulting calculations took into account the differences by socio-economic
status, social security entitlement, inclusion of medications in basic
clinical manifestations or one’s access to them through subsidized
prices, the patient’s clinical condition, etcetera.
In this way, outlays
on HIV/AIDS treatment were estimated to total US $49 million; this
figure was the result, in nearly equal parts, of out-of-pocket expenses
of patients (US $25.4 million) and of public budget expenditures (US
$24.0 million).
These outlays
include the treatment considered optimum in 1995 (essentially the
use of a combination of two antiretrovirals and prophylactic medications)
for a minority of AIDS patients (approximately 38% of the estimated
total number of survivors during that year). Asymptomatic seropositive
persons generally receive neither the antiretroviral nor the prophylactic
treatment. The treatment pattern outside of the large hospital centers
in the big cities included a higher number of days of hospitalization
and a lower use of medication.
The greater part
of the out-of-pocket expenses correspond to the use of prophylactic
medication or a second antiretroviral. Hospitalization expenses were
paid primarily by social security institutions and, secondarily, from
patients’ own funds. It is worth noting that out-of-pocket expenses¾
even though in the aggregate they account for nearly one-half of the
expenses in this item¾ in general contribute to a suboptimum pattern
of treatment for the majority of the patients; that is, this accounting
includes expenses disbursed by beneficiaries additional to those contributed
by their social security institution (e.g., nutritional supplements
in cases of wasting syndrome), and others, the majority of non-beneficiaries,
which include all expenses from those on antibiotics for prophylaxis
to those on anti-retrovirals, fundamentally, purchased in a still-insufficient
manner for a complete mono-therapy scheme.
Outlays on antiretrovirals
contributed to an annual expenditure of US $20.5 million, paid for
mainly by patients and by social security institutions. (Table 6)
Table
6. HIV/AIDS Treatment expenditures by type and source
Mexico, 1995
| |
Hospital
|
Clinic
Visits
|
Anti
retrovirals
|
Other
Pharm
|
Labora-tory
Tests
|
TOTAL
|
| PUBLIC |
4..8
(10%)
|
0.6
(1%)
|
9.9
(20%)
|
5.4
(11%)
|
3.3
(7%)
|
24.0
(49%)
|
| Direct
Government |
0.5
(1%)
|
0.2
(<1%)
|
0.2
(<1%)
|
1.2
(2%)
|
1.8
(4%)
|
3.9
(8%)
|
| Social
Security |
4.3
(9%)
|
0.4.
(1%)
|
9.7
(20%)
|
4.2
(9%)
|
1.5
(3%)
|
20.1
(41%)
|
| PRIVATE |
1.5
(3%)
|
1.1
(2%)
|
10.6
(21%)
|
7.3
(15%)
|
4.8
(10%)
|
25.4
(51%)
|
| Out
-of-Pocket |
1.5
(3%)
|
0.9
(2%)
|
10.6
(21%)
|
7.3
(15%)
|
4.8
(10%)
|
25.2
(51%)
|
| Non-
Government Organization |
0
(0%)
|
0.2
(<1%)
|
0
(0%)
|
0
|
0
|
0.2
(<1%)
|
| TOTAL |
6.3
(13%)
|
1.7
(3%)
|
20.5
(41%)
|
12.7
(26%)
|
8.1
(16%)
|
49.4
(100%)
|
The role of
governments in the prevention and care of AIDS(IV)
There are three
different roles that governments assume, in different degrees, in
the health-care sector: regulation, financing, and the provision of
health services.
Not all governments
provide health services in a direct way; all governments, however,
finance health services in varying degrees and without a doubt all
assume the regulation of anything which may cause harm or cause risk
of loss of health as an intrinsic function of the state.
The regulating
role of government in health matters is almost indisputable; however,
on the issue of financing the provision of health services, there
is much debate over which interventions should be financed. The direct
provision of service by a country’s ministry of health has been
highly questioned, particularly when comparing it to similar health
services provided by private or non-profit institutions, which operate
both in urban and in rural areas. Even so, the provision of adequate
services to the affected population should be guaranteed, both under
insurance schemes and in the case of the uninsured population.
One of the major
components of health-care cost for AIDS patients is money spent on
medication. In some Latin American and Caribbean countries, the National
AIDS Programs furnish the necessary pharmaceutical products, including
antiretroviral combinations, as well as the ambulatory and hospital
care required for all patients diagnosed with AIDS (e.g., in Chile);
in other countries that same care is furnished to all patients, provided
they are covered by a social security system. As the number of cases
increases, it is considered that both the former and the latter will
run into budgetary problems in order to be able to absorb the costs
of furnishing such care.
However, it is
necessary to highlight that the financial solution of social security
institutions is not to exclude HIV/AIDS from their treatment scheme
or to provide the affected with suboptimal treatments. Adequate actuarial
calculations will make it possible to provide care in keeping with
the advance of medical technology, not only for AIDS but also for
the care of other diseases.
It is worth noting,
however, that social security institutions mainly invest in the treatment,
frequently inadequate, of patients, and their preventive emphasis
often includes only the control of blood banks. Their actions for
the prevention of HIV sexual transmission are scant, inefficient and
insufficient. Then it is clear, in the light of the insufficiency
of preventive actions, that policies excluding the treatment of AIDS
patients are more than informed decisions, moral sanctions against
the sexual activity of the individuals.
Some alternatives
for reducing health-care costs involve the adoption of ambulatory
management schemes. Paradoxically, in places with less trained staff,
and usually on a greater scarcity of medical resources, preference
is given to hospitalization without antiretroviral treatment, resulting
in higher cost and lower effectiveness.
The most serious
problem concerns low-income patients who are not covered by any type
of insurance, private or social security, and who live in countries
in which their health-care costs will not be covered with public funds.
In these cases, such persons shall have to turn to charity health-care
schemes or enter into research protocols that normally provide, free-of-charge,
the medications under study, albeit in no way do they constitute the
optimum scheme for the provision of services to the disenfranchised
population. Unfortunately, there are few alternatives for this type
of patients, whereupon governments which do not cover these health-care
costs should foster and encourage the care of disenfranchised patients
by other mechanisms.
Despite its high
cost, the treatment for HIV/AIDS is not the most expensive of those
applied in medical and social security institutions. In this sense,
governments should establish uniform guidelines for covering the costs
of diseases among their patients, prior to eliminating resources for
the care of AIDS. The message, then, is very simple: the coverage
of diverse diseases must abide by the same guidelines of evaluation.
If the financing of heart transplants, chemotherapy in certain cancers,
bone marrow transplants or other interventions is not questioned,
then the financing of antiretroviral treatment of AIDS patients should
not be questioned.
That is to say,
Latin American and Caribbean countries, unfortunately, still do not
have sufficient resources to finance with public funds all their health
problems at a level of access and quality similar to that prevailing
in industrialized countries; therefore, in their reform processes,
they will need to set priorities for the public financing of certain
interventions over others and cover 100% of the cost of basic services
for the care of low-income populations. The major issue of discussion,
then, will lie in the definition of the basic packages and the guidelines
used for determining their inclusion.
Special care should
be taken over cost-benefit studies in the case of AIDS, since the
great advances in antiretroviral therapeutics may have increased the
costs and the benefits of its utilization.
By way of conclusion,
the government’s first responsibility is to ensure at the national
level that the blood banks are protected against the presence of HIV,
with public or private financing. Moreover, it is the government’s
obligation to guarantee for AIDS patients the same type of care that
is given to patients with other chronic diseases, under the diverse
schemes of coverage and provision of services in the countries. For
example, one of the priorities, therefore, is to establish provisions
for private insurance policies not to exclude coverage of AIDS. The
government’s regulatory responsibility in these matters is indisputable.
Likewise, the government’s intervention is necessary to stem
HIV sexual transmission. However, this is a complex matter due to
the possible interpretation of governmental actions as an intrusion
in the private life of citizens. Although it does not correspond to
the government to be the implementing agent of interventions, it is
indeed its competence to foster and ensure that specific social groups
become involved in the strategies for prevention and care.
In this sense,
one of the major recommendations arising from international conferences
on AIDS and from international agencies working on AIDS suggest that
governments perform a promoting, regulatory and financing function
of preventive interventions, by backing diverse social organizations
that can work effectively and efficiently on the subject.
Even the lack
of explicit policies is a policy. In terms of prevention and control
of AIDS, the absence of activities in this particular respect is a
policy of grave consequences in the medium and the long term
National governments
have the obligation to undertake preventive actions against HIV transmission
and to guarantee adequate care for the HIV-infected population and
for those who are ill with AIDS, because it concerns a public-health
problem. Not to do it, owing to the political costs that may be involved
therewith, constitutes, at the present moment, a grave irresponsibility,
putting in danger large sectors of the population, and thereby affecting
the life of countries from the economic and social points of view.
Medical institutions,
in turn, have the obligation to provide the best therapeutic treatment
available, for which it is necessary to implement continuing training
activities for their staff.
Regional approaches
for combating HIV/AIDS
On January 1,
1996, the new Joint United Nations Programme on HIV/AIDS (UNAIDS)
was implemented. This program is co-financed by the United Nations
Development Program (UNDP), the United Nations Educational, Scientific
and Cultural Organization (UNESCO), the United Nations Fund for Population
Activities (UNFPA), the United Nations Children’s Fund (UNICEF),
the World Health Organization (WHO); and the World Bank. The work
of UNAIDS at the world level and at the country level has three mutually
reinforcing functions: development of policies and research, technical
support, and promotion. One of the central elements of these efforts
is based on the biggest lesson learnt in the last decade: the HIV/AIDS
epidemic is not just an epidemic outbreak.(34)
The characteristics
of the HIV/AIDS transmission cause it not to display, in terms of
epidemiological control, important geographical regional differences;
rather, HIV extends beyond the boundaries of any country by multiple
mechanisms, among them, migration and tourism. That is why the regional
approach should be given overriding importance, not only in view of
the antecedents of the disease, but primarily because of the means
for its control, given the similarities in the area.
As was mentioned
in this publication’s preface, the Fundación Mexicana para la
Salud is the implementing agency of the SIDALAC initiative, which
was originally promoted by the World Bank and now is part of UNAIDS.
The general objective of SIDALAC is to contribute to the mobilization
of national and international efforts in Latin America and the Caribbean
against the AIDS and other STD epidemics, by promoting awareness among
decision makers in the region, supporting the development of a new
generation of programs for the control of AIDS, and supporting the
development of specific regional approaches for Latin America and
the Caribbean regarding the control of AIDS and of other sexually
transmitted diseases.
As a result of
this initiative, approaches are expected that, more than the sum of
individual efforts of countries, shall contain in their perspective
the notion of region, with its consequent coordination of activities
and the mutual sharing of lessons-learned in neighboring countries.
Conclusions
HIV/AIDS is spreading
at the same time that it is becoming endemic. To remain free from
infection until one reaches maturity is a challenge of great magnitude
in communities with a high HIV prevalence, since the preventive measures
have had limited success mainly because the broader context or environment
in which people live has not been appropriate for prevention.
The prevention
and the treatment of the affected have been separated artificially.
But for individuals and their families, as well as for communities,
to face HIV infection is part of a long-term challenge peculiar to
the AIDS era, a challenge which includes protecting oneself from HIV.
We must integrate the aspects of prevention and health-care in such
a way so that one can exploit the rich interface of both aspects.
More and better quality interventions are needed throughout the prevention-care
continuum. At the same time, the vulnerability of social action should
be reduced, ranging from community mobilization to international initiatives.(34)
There are two
levels of prevention: primary prevention prevents the occurrence of
new infections; and secondary prevention reduces morbidity and mortality,
once the infection is already present. Primary prevention has been
achieved with the elimination of infected blood products, antiviral
treatment to pregnant women with HIV infection, behavioral change
programs to reduce high-risk practices, consistent use of condoms,
the treatment and control of sexually transmitted diseases. Secondary
prevention is aimed at interventions that help to reduce the progression
of the HIV infection, delay the appearance of opportunistic infections
and AIDS, and increase the survival and quality of life of infected
patients. These interventions are based on timely and effective antiviral
treatment, prophylactic treatment of opportunistic infections, improving
nutrition, and managing the patient’s emotional state.
The struggle against
the social vulnerability to the HIV infection is the struggle itself
against the epidemic and corresponds to a long-term effort that is
the responsibility of the current governments, although the length
of their administration-terms may end before the beneficial effectos
of such a policy are evident.
To achieve this
objective, it is suggested to re-direct the existing resources in
the different countries through the following actions:(VI)
1. To identify
the epidemiological pattern of each country in order to determine
populations at increased risk for HIV.
2. To identify
civil and social groups and organizations that work currently with
such populations.
3. To promote
and strengthen such organizations for them to implement community-based
prevention and care interventions, respecting the characteristics
and specificities that such programs would need.
In their role
of regulation of health and education policies, governments could
implement such actions immediately through some or all of the following
mechanisms:
1. Creation of
a technical group composed of authorities, scholars and members of
civil organizations, which would call for prevention projects against
HIV, to be financially supported, after their assessment.
2. The role of
this technical group would be to approve the proposals within an open
contest, based on their quality.
3. To evaluate
the proposals of groups in terms of the capability of organizations
to account for the cost-effectiveness of their designs, their population
coverage, and the recognized quality of work already carried out,
as well as the theoretical base of the research and intervention proposals.
4. To implement
coordination mechanisms with organizations, such as, institutional
development, tax exemption mechanisms, agreements with social groups,
or contracts or subcontracts, etcetera.
The strategy of
involvement and coordination with civil and community organizations,
combined with an overall public health and education policy, seems
to be the most efficient to decrease virus transmission in a permanent
and consistent manner. Social marketing has shown certain effectiveness
in behavior change, but ephemeral. The costs of sustaining this kind
of campaigns are too high and distract resources for other interventions
of longer-term effectivity.
However, immediate
actions are also required in order to know the impact of the epidemic
and carry out preventive interventions. For this reason, it is suggested
that governments commission a series of studies whose goals should
be:
1. To carry out
diagnosis of new infections.
2. To determine
the future course of the epidemics and the subepidemics, and to determine
those groups in urgent need of interventions.
3. To investigate
quantitatively and qualitatively the structural determinants of the
vulnerability of such groups to HIV infection and to inquire into
the effectiveness of intervention models designed with the information
produced by the studies described above.
---------------------------------------
I This section
is based on Chapter 2 of this publication, "Current State of Knowledge
in Basic Sciences on HIV/AIDS" written by Luis Soto.
II This section
is based on Chapter 3 of this publication, "Clinical Aspects of HIV
Infection. Current Concepts 1996", written by Juan Sierra.
III This section
is based on Chapter 4 of this publication, "Epidemiology and Public
Health", written by Carlos Avila-Figueroa.
IV This section
is based on Chapter 6 of this publication, "HIV/AIDS and Economic
Development", written by Enrique González.
V This section
is based on Chapter 7 of this publication, "HIV/AIDS and the Reform
of the Health Care Systems of Latin America and the Caribbean", written
by Jorge Saavedra.
VI This section
is based on Chapter 5 of this publication, "Social Sciences and AIDS",
written by Ana Amuchástegui-Herrera.
References
1. Bacchetti P,
Moss AR. Incubation Period of AIDS in San Francisco. Nature 1989;338:251.
2. Volberding
PA, Lagakos SW, Koch MA, et al. Zidovudine in asymptomatic human immunodeficiency
virus infection: a controlled trial in persons with fewer than 500
CD4 postitive cells per cubic millimiter. N Engl J Med 1990; 322:941-949.
3. Soto-Ramírez
LE, Renjifo B, McLane M, et al. HIV-1 Langerhans’ Cell Tropism
Associated with Heterosexual Transmission of HIV. Science 1996;271:1291-1293.
4. Mann JM.
Human rights and AIDS: the future of the pandemic. Gac Med Mex 1996;
132 Suppl 1. S13-S20.
5. Gottlieb MS,
Schroff R, Schauker HM et al. Pneumocystis carinii pneumonia
and mucosal candidiasis in previously health homosexual men: evidence
of a new acquired cellular immunodeficiency. N Engl J Med 1981; 305:1425-31.
6. Centers for
Disease Control. Pneumocystis pneumonia-Los Angeles. MMWR 1981;30:250-2.
7. Centers for
Disease Control. Immunodeficiency among female sexual partners of
males with acquired immunodeficiency syndrome (AIDS) - New York. MMWR
1983;31:697-8.
8. Centers for
Disease Control. Unexplained immune-deficiency and opportunistic infections
in infants - New York, New Jersey. MMWR 1982; 31:665-7.
9. Centers for
Disease Control. Possible transfusion-associated acquired immune deficiency
syndrome (AIDS) - California. MMWR 1982;31:652-4.
10. Soto L. "Current
State of Knowledge in Basic Sciences on HIV/AIDS". In: Izazola JA,
ed. AIDS: An update. Mexico City:FUNSALUD/LIMUSA, 1996.
11.Shilts R. And
the band played on. Politics, people and the AIDS epidemic. New York:
St. Martin’s Press, 1987.
12. Sierra J.
"Clinical Aspects of HIV Infection. Current Concepts 1996" In: Izazola
JA, ed. AIDS: An update. Mexico City:FUNSALUD/LIMUSA, 1996.
13. Volkow P.
"Comentarios a las ponencias: La Calidad de la Atención Médica de
Pacientes con SIDA y La atención de pacientes con SIDA en el IMSS".
Gac Med Mex 1996; 132 suppl 1. S73-S74.
14. Avila C. Epidemiology
and Public Health. In: Izazola JA, ed. AIDS: An update. Mexico City:FUNSALUD/LIMUSA,
1996.
15. Zacarias F.
El SIDA en el Mundo. Gac Med Mex 1996; 132 Suppl 1. S25-S28.
16. UNAIDS. Fact
sheet. 1 July 1996. Geneva: UNAIDS, 1996.
17. Izazola-Licea
JA. El Impacto del SIDA en América Latina: Hacia un enfoque regional.
Gac Med Mex 1996; 132 Suppl 1. S29-35.
18. Murray CJL,
Lopez AD, & Jamison D.T.. The global burden of disease in 1990:
summary results, sensitivity analysis and future directions. In: C.J.L.
Murray & A.D. Lopez eds. Global comparative assessments in the
health sector. Disease burden, expenditures and intervention packages.
World Health Organization, Geneva: 1994; 97-138.
19. Organización
Panamericana de la Salud/ Organización Mundial de la Salud. Vigilancia
epidemiológica del SIDA en las Américas. Informe Trimestral 10 de
marzo de 1996. OPS/HCA/96.004. Información disponible en internet
http: //www.paho.org.
20. Izazola-Licea
JA, Valdez-García M, Sánchez-Pérez HJ, del Río-Chiriboga C. La mortalidad
por el SIDA en México de 1983 a 1992. Tendencias y años perdidos de
vida potencial. Salud Publica Mex 1995:37:140-148.
21. Consejo Nacional
para la Prevención y Control del SIDA (CONASIDA). Situación epidemiológica
del SIDA. Datos actualizados hasta el primer trimestre de 1996. SIDA-ETS
(México)-Separata 1996;2:Num. 1:I-XX. Información disponible en internet
http://cenids.ssa.gob.mx//
22. Hessol NA,
Buchbinder SP, Colbert D, et al. Impact of HIV infection on mortality
and accuracy of AIDS reporting on death certificates. Am J Public
Health. 1992;82:561-564.
23. Buehler JW,
Devine OJ, Berkelman RL, Chevarley FM. Impact of the Human Immunodeficiency
Virus epidemic on mortality trends in young men, United States. AJPH
1990;80:1080-1086.
24. Stein M, O’Sullivan
P, Wachtel, et al. Causes of Death in persons with Human Immunodeficiency
Virus infection. AJ of Medicine 1992;:93:387-390.
25. Amuchastegui
A. Social sciences and AIDS. A state-of-the-art review for
Latin America and the Caribbean after the XI International Conference
on AIDS. Mexico City:FUNSALUD/LIMUSA, 1996.
26. Vandale S.
Mujeres y vulnerabilidad para el VIH: perspectivas para la prevención.
In: Izazola JA, ed. AIDS: An update. Mexico City:FUNSALUD/LIMUSA,
1996.
27. Volkow P.
"Women and HIV/AIDS". In Izazola, J.A. (ed). AIDS: The state of the
Art. Mexico City: FUNSALUD/LIMUSA, 1996.
28.González E.
HIV/AIDS and Economic Development. In: Izazola JA, ed. AIDS: An update.
Mexico City: FUNSALUD/LIMUSA, 1996.
29. The World
Bank. World Development Report 1993. Investing in Health. New York:
Oxford University Press; 99-107.
30. Hillman AL.
Cost-effectiveness: from whose perspective? JAIDS and Human Retrovirol
1995; 10(suppl 4): S14-S18.
31. Schulman KA,
Lynn LA, Glick HA, Eisenberg JM. Cost effectiveness of low-dose zidovudine
therapy for asymptomatic patients with human immunodeficiency virus
(HIV) infection.. Ann Interen Med 1991:114:798-802.
32. del Río C.
Tratamientos para el SIDA y padecimientos asociados: costo y efectividad.
Gac Med Mex. 1996; 132 Suppl 1. S77-S82.
33. Shepard D,
et al. Expenditures on HIV/AIDS: Levels and Determinants, Lessons
from five countries. Presented in: The World Bank, the European Copmmission
and UNAIDS. "AIDS and development: the role of government". Chateu
de Limelette, Limelette, Belgium, June 17-19, 1996.
34. Izazola-Licea
JA, Saavedra J, Prottas J, Shepard D. Levels and determinants of expenditures
on the treatment and prevention of HIV/AIDS in Mexico. Presented in:
the World Bank, the European Commission and UNAIDS. "AIDS and development:
the role of government". Chateu de Limelette, Limelette, Belgium,
June 17-19, 1996.
35. Cowal SG.
UNAIDS: Toward an expanded response to the HIV/AIDS pandemic. Gac
Med Mex 1996; 132 Suppl 1. S21-S24..
|